Causes of Burns
The pie chart below and associated graph illustrate the most common etiology or causes of burns.

Does this look familiar? That's because it was also in last week's blog post but that doesn't make it any less important. We can learn a number of important of facts from this graph. First, notice that fire/flame injuries are the most common cause of burns, followed closely by scald injuries. Second, consider the different causes of burns. Prior to my research, I had not considered chemical burns at all. Knowing the cause of a burn can greatly influence the type of treatment that a burn will require. Lastly, recognize the category of skin disease is not representative of a type of burn. These statistics above reflect the number of cases handled by burn centers. Burn units often treat skin disease such as stevens-johnson syndrome or TENS (toxic epidermal necrolysis syndrome), for example, because of burn units are accustomed and prepared to deal with extreme cases of skin damage and its associated complications.
Systemic Response
As a result of large-scale burns there are a number of systematic complications that often take place. Within the first hours of a burn capillary permeability will increase drastically causing a major loss of intravascular contents. These fluids accumulate in the interstitial spaces and will cause edema. This loss of vascular contents also cause patients to become very hypovolemic and suffer from very low blood pressure. These changes in vascular volume also can lead to a lack of perfusion to vital organs. For these reasons, it is obvious why burn patients undergo aggressive fluid replacement in the hours following their burn.
In addition to complications related to vascular permeability and vascular volume, burn patients can also suffer from respiratory and metabolic complications. When the body is burned, inflammatory mediators are released which add to the inflammation response and edema but these mediators can also cause constriction of the bronchioles resulting in respiratory distress syndrome.
The body's basal metabolic rate also increases drastically as a result of large burns. Because of this increase in metabolic rate, burn patients often undergo aggressive enteral feedings in order to preserve the digestive system from damage (Hettiaratchy et al. par 3).
Cardiac function can also be a major problem for burn patients. Changes in cardiac function are largely due to the changes in vascular volume but it is also thought that cardiac contractility is decreased due to the release of tumour necrosis factor alpha (TNF-alpha). TNF-alpha is released as a result of large scale burns and can be detected in the blood. Although, it seems that TNF-alpha is not initially elevated in large scale burns but instead appears after initial admission to a hospital (one hour post burn in one study I looked at). Defects in the heart contractility appear around eight hours post burn (Maass et al abstract). For more information on TNF-alpha in relation to burns please follow the below link and associated journal article.
Renal failure in burn patients is a complicated process as it is often a result of many compounding factors. Acute renal failure can be due to decreased perfusion of the kidneys because of hypovolemia and decreased cardiac output. Respiratory failure can also result in renal failure because of a lack of oxygen reaching the kidneys. Additionally, burns cause release of large amounts of inflammatory mediators, denatured proteins, and stress related hormones that can damage or suppress the kidneys. Nephrotoxic (kidney damaging) substances are often used in the treatment of burns. For example, many antibiotics used to fight the substantial risk of infection are harmful to the kidneys. Lastly, infection can also cause kidney failure (Emara et al. par 5-12).
Finally, infection is a major risk factor for burn patients. When the integrity of the skin is compromised the body is very vulnerable to infection. To make this worse, the body's immune response is suppressed as a result of the trauma that the skin has sustained and resulting inflammatory response. Also, the intestines become more permeable due to the inflammatory response which allows natural flora in the intestines to migrate into the surrounding tissues (Farina et al. par 1).
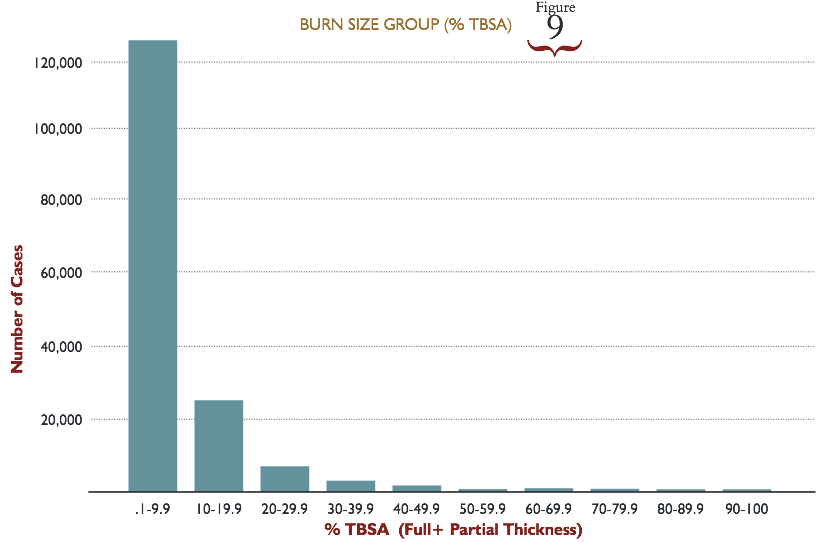
According to Hettiaratchy et al., once a burn has reached 30% TBSA or more these burn complications become systemic.
Obviously, the systemic burn response is a complicated and intertwined process. Hopefully, this is a helpful outline of some of the more common complications with burns. In upcoming weeks, I plan on expanding on these concepts and perhaps addressing the treatments associated with each.
Works Cited
Emara, S.S., and A.A. Alzaylai. “Renal Failure in Burn Patients: A Review.”
Annals of Burns and Fire Disasters 26.1 (2013): 12–15. Print.
Hettiaratchy, Shehan, and Peter Dziewulski. “Pathophysiology and Types of Burns.” BMJ : British Medical Journal 328.7453 (2004): 1427–1429. Print.
Jayme A. Farina Jr., Marina Junqueira Rosique, and Rodrigo G. Rosique,
“Curbing Inflammation in Burn Patients,” International Journal of
Inflammation, vol. 2013, Article ID 715645, 9 pages, 2013.
doi:10.1155/2013/715645
Maass, David L., Dixie Peters Hybki, Jean White, and Jureta W. Horton.
"The Time Course of Cardiac NF-κB Activation and TNF-α Secretion by
Cardiac Myocytes After Burn Injury: Contribution to Burn-Related Cardiac
Contractile Dysfunction." Shock 17.4 (2002): 293-99. Print.